
Remember me



Discover is a real-world database of linked primary and secondary electronic health records covering 2.8 million people residing in north-west London, UK, accounting for more than 95% of the north-west London population [10]. The database is linked to the Whole Systems Integrated Care database, which was developed for commissioning and direct patient care across north-west London [11]. Primary care data are available from 1 January 2004 onwards, whereas secondary care linkage and mortality data are available from 1 January 2015. Discover is representative of the UK population with regard to age and sex, but is more diverse in terms of ethnicity [11].
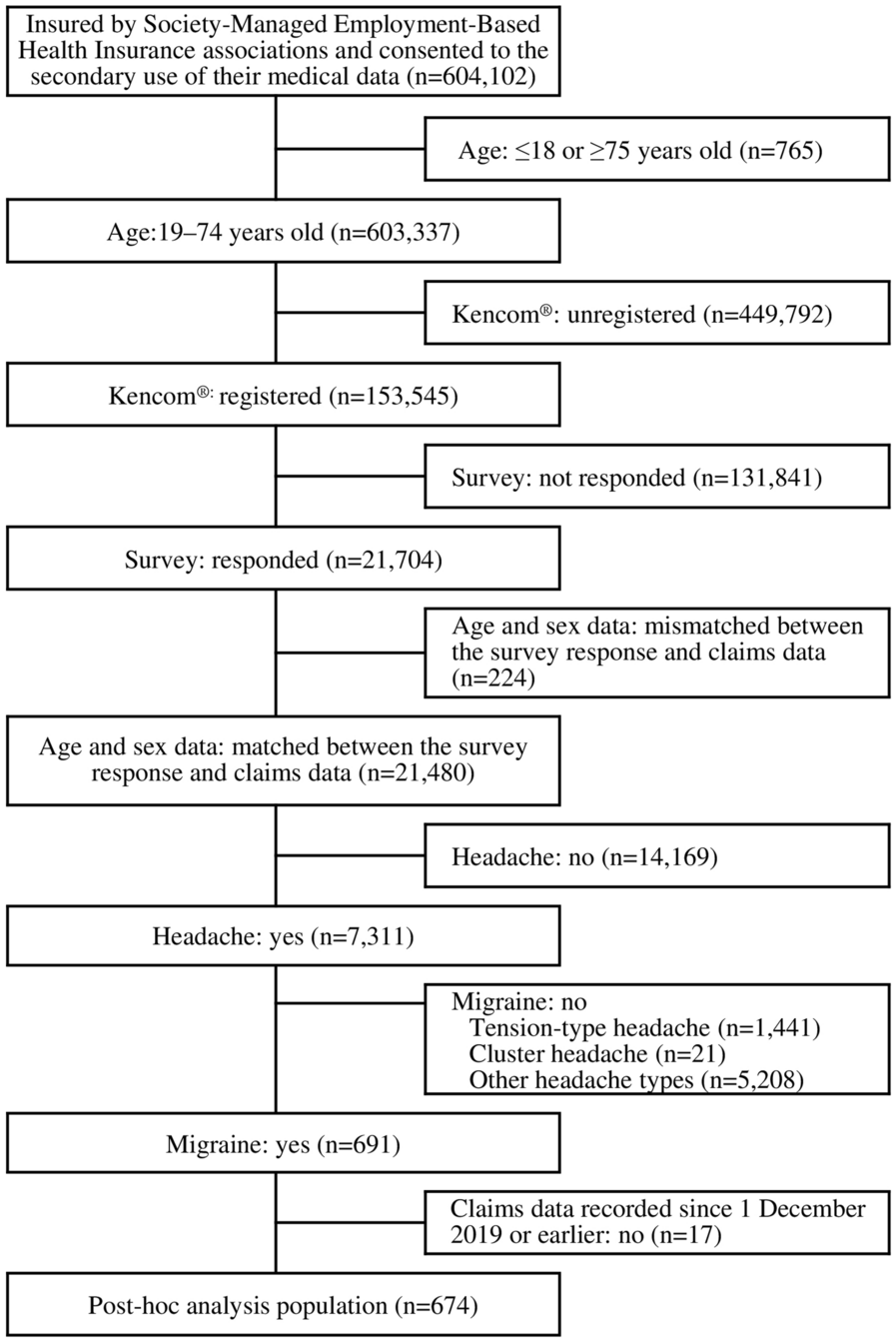
Study Design and PopulationThis was a retrospective open cohort study using data from eligible individuals between 1 January 2010 and 31 December 2019 (Fig. 1). Individuals aged 18 years and older were included if they were eligible for bariatric surgery according to the National Institute for Health and Care Excellence (NICE) criteria [BMI ≥ 40.0 kg/m2 (obesity class III), or 35.0–39.9 kg/m2 (obesity class II) and a diagnosis of an ORC]. Black and Asian populations have lower BMI thresholds for obesity [12]. Therefore, specific thresholds of ≥ 37.5 kg/m2, or 32.5–37.4 kg/m2 plus an ORC were applied for individuals of Black or Asian ethnicity [12]. The index date was the date on which an individual met all the required entry criteria. For example, if an individual had an ORC diagnosis that occurred up to 3 years after an eligible BMI entry, the index date would be the date of the ORC diagnosis. Individuals were followed from index date until death, leaving the database or the end of the study period, whichever occurred first.
Fig. 1
Study design. BaS bariatric surgery, BMI body mass index, GP general practitioner, ORC obesity-related complication
Individuals entered the bariatric surgery treated population during follow-up if they had a diagnosis code for bariatric surgery in primary care records, or a hospital attendance with a surgery code for bariatric surgery in secondary care records, in the post-index period.
The ORCs considered to indicate eligibility for bariatric surgery in individuals with eligible BMI measurements were asthma, atherosclerotic cardiovascular disease, dyslipidaemia, gastro-oesophageal reflux disease, hypertension, idiopathic intracranial hypertension, non-alcoholic fatty liver disease (with or without steatohepatitis), obstructive sleep apnoea, osteoarthritis, polycystic ovary syndrome, type 2 diabetes and urinary incontinence. Records of these ORCs were valid on, before or up to 3 years after eligible BMI measurements. The rationale for the choice of these ORCs was based on the link between risk of these conditions and higher BMI, the inclusion of these in previous analyses using Discover data [13, 14] and for alignment with the relevant NICE guidance on conditions that may be improved by bariatric surgery [12].
ORCs and surgery codes were identified in primary or secondary care records using International Classification of Diseases, Tenth Revision (ICD-10) codes, Office of Population Censuses and Surveys 4th revision (OPCS-4) codes and Read codes for primary care data (Supplementary Tables S1 and S2).
Individuals with no record of general practitioner (GP) or nurse practitioner activity for more than 5 years during the study period and those who had undergone bariatric surgery at any time before index date were excluded from the study. Other exclusion criteria were a record of stomach cancer less than 5 years before bariatric surgery, a record of gastric balloon or bubble procedures, evidence of more than 10% weight loss before bariatric surgery (i.e. a BMI measurement occurring after maximum BMI measurement and more than 10% below the maximum measurement) or, for individuals who did not undergo bariatric surgery, weight loss of more than 10% that meant their BMI fell outside the criteria for inclusion.
Outcomes in the Population Who Received Bariatric SurgeryTime to Bariatric Surgery and Baseline CharacteristicsIndividuals who received bariatric surgery were stratified by the time between becoming eligible for bariatric surgery and undergoing surgery (< 2 years, 2–3.9 years or ≥ 4 years). Baseline characteristics, including age, sex, ethnicity and BMI, were compared between these categories.
Healthcare Costs Between Index Date and Date of SurgeryTotal direct healthcare costs (costs of primary and secondary healthcare interactions, plus prescription costs) were assessed at 1-year intervals between the index date and date of surgery and compared between the groups stratified by time to bariatric surgery.
Primary care included all appointments across primary care (GP consultations and nurse practitioner appointments); costs were derived from Personal Social Services Research Unit data from 2020 [15]. Inpatient admissions (admitted patient care), outpatient care and emergency department visits were identified from records of secondary care interactions, with costs derived from the Secondary Uses Service produced by NHS Digital. Prescription costs were calculated using net ingredient costs, obtained from the national report on the net ingredient cost of all prescriptions dispensed in England [16]. Costs were age standardized to the European Standard Population and were adjusted to 2019 costs using UK Consumer Price Index inflation data from the Office for National Statistics.
Descriptive data are presented as mean and standard deviation (SDs) or as median (interquartile range) for continuous variables, and as number and percentage for categorical variables.
Estimated Effect of Modelled Weight Loss on BMI and CostsIndividuals in the bariatric surgery eligible cohort who had been eligible for surgery for more than 1 year and who had at least 1 year of follow-up after index were included in an analysis modelling the estimated impact of weight loss on BMI, transition between BMI groups and healthcare costs over 2 years. This time horizon was chosen to reflect the approximate waiting time for bariatric surgery in the UK, which varies between 12 and 24 months or more across NHS trusts, depending on local funding and service availability. Therefore, our analysis indicated the potential cost savings that could be achieved in the absence of delays to bariatric surgery or other weight loss methods.
To estimate the impact of weight loss, four weight loss scenarios were applied at index date: 10%, 15%, 20% and 25% weight loss. All weight loss was assumed to occur during year 1, following a linear trend, with maintenance of this weight loss during year 2. For example, for the 10% weight loss scenario, the average modelled weight loss in the first year was 5%, with 10% weight loss achieved by the end of year 1 and maintained during year 2. The modelling assumptions for weight loss were independent of the weight loss method and did not include any costs or other assumptions relating to surgery or obesity management medication.
For the bariatric surgery eligible population, costs used in the modelled weight loss analyses were derived from the data used in the current study, and for obesity class I (30.0–34.9 kg/m2) and overweight (25.0–29.9 kg/m2) costs were derived from populations included in previous analyses using Discover data [13, 14]. Healthcare costs were age standardized to the European Standard Population and were assumed to differ between BMI groups based on ORC profiles. In brief, the eligible population for the analysis was stratified according to the highest-cost ORC at index, allowing a weight to be assigned to each ORC. Costs for each BMI group were then estimated by applying the ORC weights to the healthcare costs incurred by individuals in each BMI group who had these ORCs. Using these assumptions, the mean healthcare cost per person per year was estimated as £1187 for the overweight group, £1254 for the obesity class I group and £1662 for the group eligible for bariatric surgery. Using these costs, and assuming that the ORC profile at index was maintained, costs were calculated for each weight loss scenario based on individuals moving to lower BMI groups following weight loss.
Estimated cost reductions for the study population across the full study period were calculated, based on aggregate cost estimates over 2 years for all eligible individuals with at least 1 year’s follow-up at any point in the whole study period. In total, there were nine eligible 2-year periods during the study. Mean estimated cost reductions for weight loss modelled over an average 2-year period are presented in this article, in addition to aggregate cost reductions for the whole study period.
Ethical ApprovalThis study was a retrospective analysis of secondary de-identified data and was not considered to be human subject research; therefore, ethics committee approval was not required. Access to the Discover dataset is managed by Imperial College Health Partners with the North West London Information Governance Committee (SDRAG) approving applications. The current analysis was conducted under approved application ID 183.
Comments (0)