
Remember me



This retrospective database analysis was conducted using 100% Medicare Limited Data Set (LDS) administrative claims data from January 1, 2017, to March 31, 2021. The LDS standard analytical files include de-identified beneficiary-level data such as enrollment, age, sex, race, region, International Classification of Diseases, Tenth Revision (ICD-10-CM), diagnosis and procedural codes, claim dates, and dates of death. LDS contains information for both institutional and non-institutional providers; the data set is available to health services researchers to examine a variety of epidemiological and economic questions of interest [22,23,24]. The limited nature of LDS stems from the fact that it does not include prescription drugs, physician claims, or durable equipment claims in comparison with other Medicare data sets such as Research Identifiable Files.
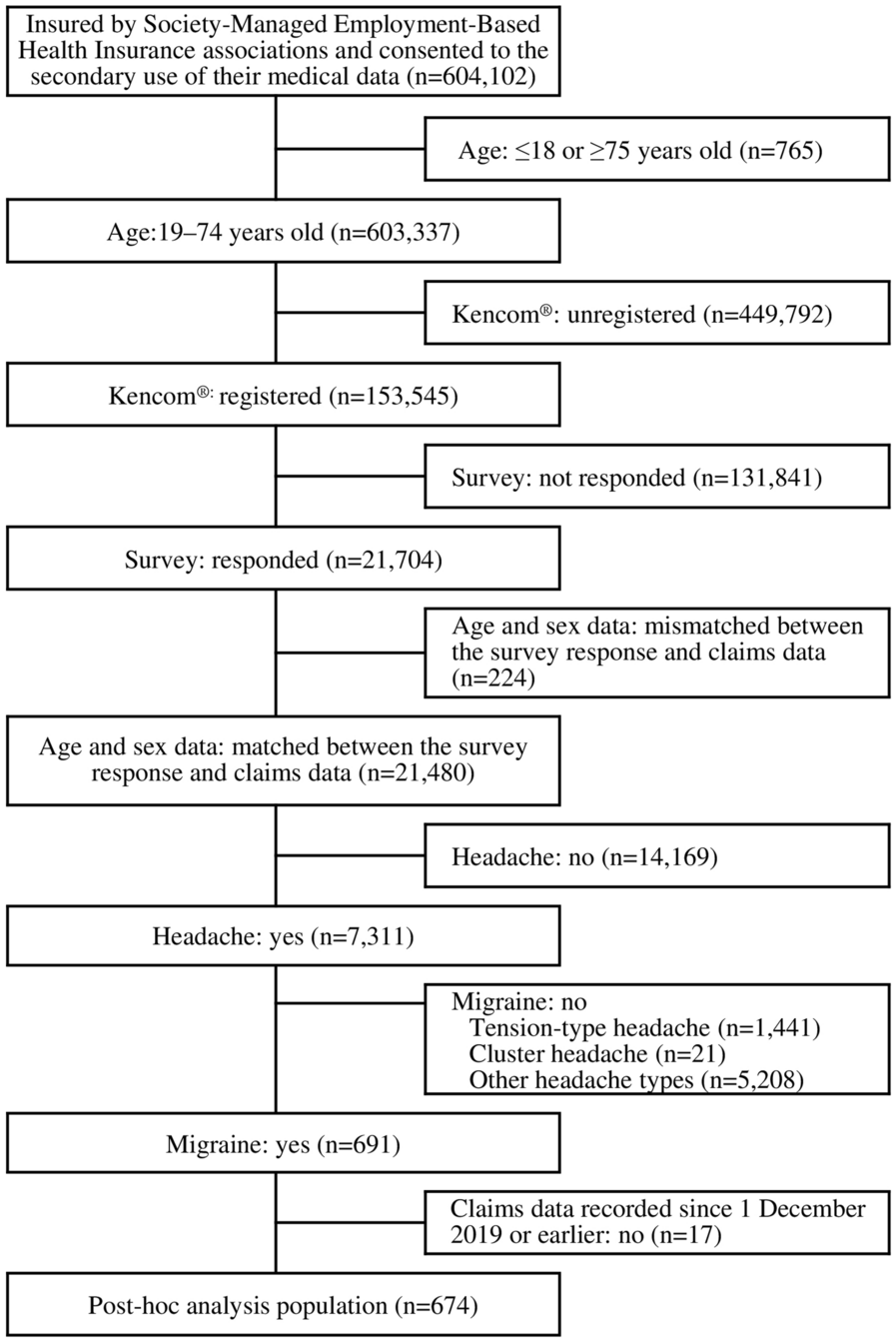
Patient Selection and Study DesignEligible patients identified for inclusion were Medicare beneficiaries aged 18 years or older, categorized as those with postsurgical chronic HypoPT and those without HypoPT (the non-HypoPT control group). Inclusion in the postsurgical chronic HypoPT group required at least two claims with a HypoPT diagnosis code (ICD-10-CM E200, E208, E209, or E892). The first diagnosis had to have occurred after thyroidectomy, parathyroidectomy, goiter removal, excision procedures on the parathyroid, or resection of the thyroid gland, which were identified by CPT or ICD-10 codes, as shown in the Supplementary Material (Table S1); the date of that claim served as the index date. The second claim had to have been made 6–12 months from the index date in the patient identification period (July 1, 2017–March 31, 2020) and served as a confirmatory diagnosis of chronic disease. At least one claim of a related surgical procedure in the 6-month baseline period prior to the index date (first HypoPT diagnosis) was required to confirm that the HypoPT was postsurgical. Patients were excluded if they had a previous diagnosis of HypoPT in the baseline period. A total of 1166 individuals with postsurgical chronic HypoPT were ultimately included in the study (Fig. 1).
Fig. 1
Study sample selection. CV cardiovascular, HypoPT hypoparathyroidism, URTI upper respiratory tract infection, UTI urinary tract infection
Individuals included in the non-HypoPT control group (N = 11,258) could not have a HypoPT diagnosis in the study period but had to have at least one medical claim in the patient identification period. For this group, a synthetic index date was assigned on the basis of the distribution of time between their first medical claim of any kind and the index date as observed among individuals with postsurgical chronic HypoPT. Namely, the synthetic index date among individuals without postsurgical chronic HypoPT was calculated by adding the time difference described above, borrowed from their matched case with HypoPT, to the date of their own first medical encounter observed during the study period.
Continuous enrollment in Medicare for at least 6 months before and 12 months after the index date was required for inclusion. The observation period of all patients in the analysis was until death, the end of Medicare enrollment, or the end of the study period (March 31, 2021), whichever came first.
Ethical ApprovalAs a result of the de-identified nature of the retrospective data set, the study did not require ethics committee review. Permission for reuse of the Medicare 100% Limited Data Set was granted by its owner.
Patient and Baseline CharacteristicsVariables considered in this study included baseline sociodemographic characteristics (age, gender, race, and Census region), and clinical characteristics (Charlson Comorbidity Index [CCI] score, CV complications, infections, renal complications, mental ill-health, fractures, cataracts, hypocalcemia, and neurological complications).
Study OutcomesStudy outcomes included four domains of complications: CV events (composite domain as well as individual risk of component acute myocardial infarction (ICD-10 code I21), congestive heart failure, cerebrovascular disease, arrhythmia, ischemic heart disease), renal complications (composite domain as well as individual risk of component nephrocalcinosis, nephrolithiasis, and stage 3–5 CKD), urinary tract infections (UTIs), and upper respiratory tract infections (URTIs). These complications were assessed via ICD-10 codes, as shown in the Supplementary Material (Table S2). All-cause mortality was also examined as an outcome.
Statistical AnalysisAnalyses of all study objectives were conducted among unmatched and matched cohorts and compared with their respective control groups. An exact matching algorithm allowing for a variable ratio between the number of matched treated and control patients [25, 26] was used to balance individuals with postsurgical chronic HypoPT and controls on age, gender, race, region, CCI score (categorical), and index year. A matching ratio of 1:2 of cases to controls was chosen to optimize the retention of sample size while balancing baseline characteristics.
The overall unmatched and matched cohorts from each patient group were used to assess mortality. In contrast, to examine the incident risk of long-term complications, four subcohorts were assembled from the full patient groups for the assessment of the incident risk of CV events, renal complications, UTIs, and URTIs (Fig. 1). To achieve this, individuals who experienced the respective complication in the baseline period were excluded for each subcohort (i.e., for the examination of incident CV event risk, patients with CV event at baseline were first excluded). Within each subcohort, matching was also performed to create two comparable groups of individuals with postsurgical chronic HypoPT and non-HypoPT controls using the same matching method as described above.
Within the unmatched and matched cohorts, Kaplan–Meier analysis was used to describe the time to event for individuals with postsurgical chronic HypoPT and non-HypoPT controls; hazard ratios for the risk of complications and death were reported on the basis of Cox proportional hazards models.
Sensitivity AnalysisThe time-to-event analysis described above was repeated with 3-month washout periods after the index date, where patients with an event during the specified washout period were censored at that point. This was done as a sensitivity analysis to examine the impact on the risk of complications as earlier events after index may be less likely to be due to a HypoPT diagnosis.
Comments (0)